



House Republicans took the first step this week toward enacting the Trump administration’s budget plan, passing a resolution to make $2 trillion in spending cuts to offset a planned $4.5 trillion in tax cuts.
The resolution puts a big bullseye on Medicaid spending, which is overseen by the Energy and Commerce committee. The committee must identify $880 billion in cuts over 10 years, and most of that would have to come from Medicaid.
It’s too early to know how slashing Medicaid will play politically. Medicaid is popular with the public (see below); some Republicans correctly fear voter backlash, and I don’t expect a single Democrats will support slashing Medicaid funding.
Nor should they. Medicaid funds essential health care services for more than 70 million lower-income Americans. Many are lower-income working people gained Medicaid coverage through the Affordable Care Act.
Medicaid also is critical for older adults. The program funds health and long-term care for over seven million Americans age 65 and older and nearly eleven million from ages 50 to 64. Justice in Aging, a national advocacy organization focused on senior poverty, notes:
Medicaid coverage is particularly important for older adults who need services not covered—or not adequately covered—by Medicare. Specifically, Medicaid is vital for older adults who need assistance with daily activities such as eating, bathing, dressing, and getting in and out of bed. The long-term assistance that they need, whether provided at home or in a nursing home, is typically paid for by Medicaid, and not Medicare. In fact, more than 6 in 10 nursing home residents rely on Medicaid.
Medicaid also helps over 12 million older adults and people with disabilities pay their Medicare premiums and out of pocket costs. “Dually eligible” Medicaid and Medicare beneficiaries live on limited fixed incomes with few assets. This is part of the at-risk population I described in my recent New York Times column on managing out-of-pocket costs in Medicare. These folks would not be able to afford Medicare without Medicaid assistance.
Unlike Medicare, Medicaid is funded jointly by the federal government and states. Federal reductions could be made through a number of mechanisms, including “block grants” or “per capita caps.” In either scenario the federal dollars sent to states would be reduced, forcing states to make tough choices about how they allocate funds. Older adults would be harmed by lost eligibility and services, unaffordable financial obligations, and a reduced quality of care.
Justice in Aging notes three ways arbitrarily capping the federal funding levels would be unfair - and I want to quote this at length to convey the depth of potential damage:
Coverage would no longer be based on medical necessity. Like Medicare and other health insurance programs, Medicaid covers health care needs based on medical necessity. However, under a fixed funding level system, medical necessity would often be superseded by external financial considerations, as the capped federal reimbursement would require states to impose significant cuts on eligibility, coverage, or both. Federal Medicaid funding would be insufficient to meet enrollees’ needs, which would result in states denying coverage for medically necessary services and vital programs such as Medicaid HCBS.
State Medicaid programs would be prevented from making necessary improvements. By using previous years’ Medicaid expenses as a base for the cap, there is an implicit assumption that the state’s expenses during those years were in the proper proportions. This assumption, however, may well be incorrect. If previous years expenses were inadequate to meet need, increased payments now may simply indicate a state’s efforts to bring its Medicaid program up to necessary standards. If, for example, a per capita cap had been in place from 2019 to 2022, 35 out of 41 states would have exceeded their cap and been forced to cover significantly higher costs.[10] Even with a higher growth rate for enrollees age 65+, 28 states would have exceeded the cap for older adults within three years. An additional eight states (36 total) would have exceeded the higher growth rate cap for people with disabilities.
Federal funding won’t keep up with rising health care needs of an aging population. A cap system also fails to account for aging of the population. Consider a state’s “aged” eligibility category, composed of persons age 65 or older. If more older individuals enroll in coverage, or the average age of enrollees increases, the health care needs of the Medicaid population would increase. Caps on funding, however, would not take the changed beneficiary population into account. Similarly, the Medicaid population could increase due to natural disaster, recession, a public health emergency, or other factors. In these circumstances, a state would be financially penalized and likely cut services to account for the reduced funding.
Long-term care and skilled nursing providers are bracing for the possible impacts. Hospitals, nursing home services and personal care services providers would be the most affected, according to Skilled Nursing News. Here’s what Linda Couch, senior Vice President of policy Leading Age had to say:
“All changes being considered in Congress are intended to limit the federal government’s financial obligation; they would shift significant costs to states that could, in turn, have a number of possible downstream effects such as provider reimbursement reductions, decreases in covered populations, or cuts to covered services in optional programs,” Couch told SNN. “Most states nor their residents nor their provider communities, including our nonprofit, mission-driven nursing home members, can sustain significant cuts in an already under-resourced system.”
All of this could be coming against a backdrop of a major crackdown by the Trump administration on undocumented workers that could hollow out the long-term care workforce. About 27 percent of care workers are immigrants, although the percentages vary by region. A shrinking number of available workers could push up labor costs in certain parts of the care sector, although market dynamics don’t always apply. Unlike typical markets where employers can raise wages to attract more workers, long-term care providers depend on Medicaid reimbursement rates, which are set by state and federal policies rather than market conditions. If those rates are too low, providers can't raise wages, even if demand for workers is high.
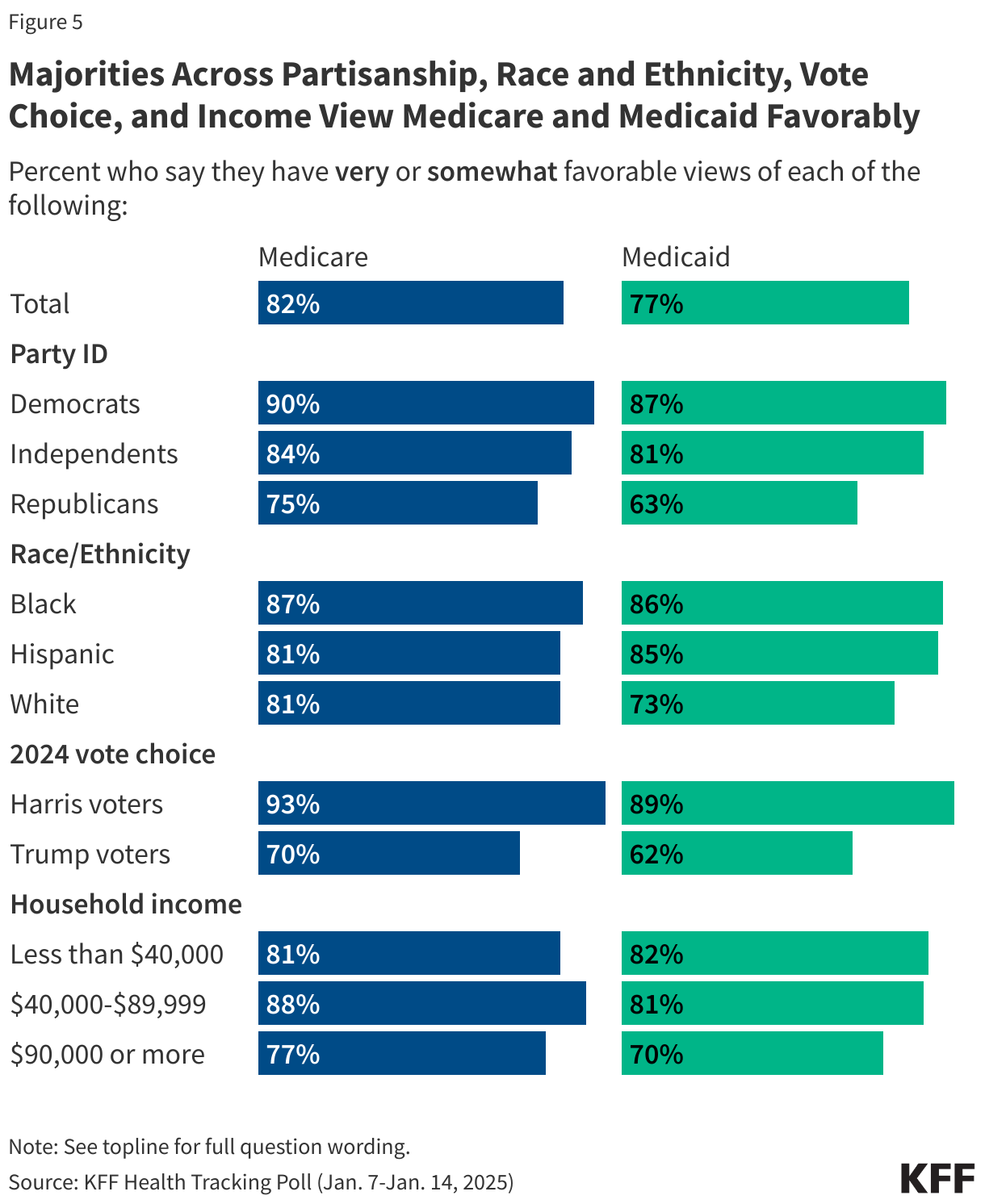
How about the politics of slashing Medicaid? It won’t play well, according to the latest KFF health care polling. It finds that 77% of Americans have a positive view of Medicaid, and that support has ticked upward in recent years:

What’s more, support for Medicaid is fairly broad across different segments of American society:
Interestingly, about half of the public thinks the federal government isn’t spending enough on either of these programs, according to KFF.
What about the tax cuts in this plan?
Taxes would be cut across the board, but wealthy households would benefit most. The plan also would increase the federal deficit. Taken together, those two aspects of the plan could ratchet up inflation - so that argues against any further interest rates cuts.
Mix in the threat of inflationary tariffs, and it’s no wonder consumer confidence is falling.
What I’m reading
The Department of Justice is investigating Medicare billing practices at UnitedHealthcare . . . Acting Social Security chief was being investigated when Trump tapped him to run the agency.